What psychologists, counselors, and physical therapists can learn from new research on using touch to teach orientation and mobility for people who are deaf blind.
/When a person with combined hearing and vision loss is tasked with learning to navigate in the real world of traffic and public transportation, many fears and risks can be expressed. As a healthcare provider, helping people evaluate the reality of fears and risks, it can be difficult to know what to say. For years there was no validation thats safe independent travel could be achieved. Or how to convey the needed information in the midst of constantly changing environments.
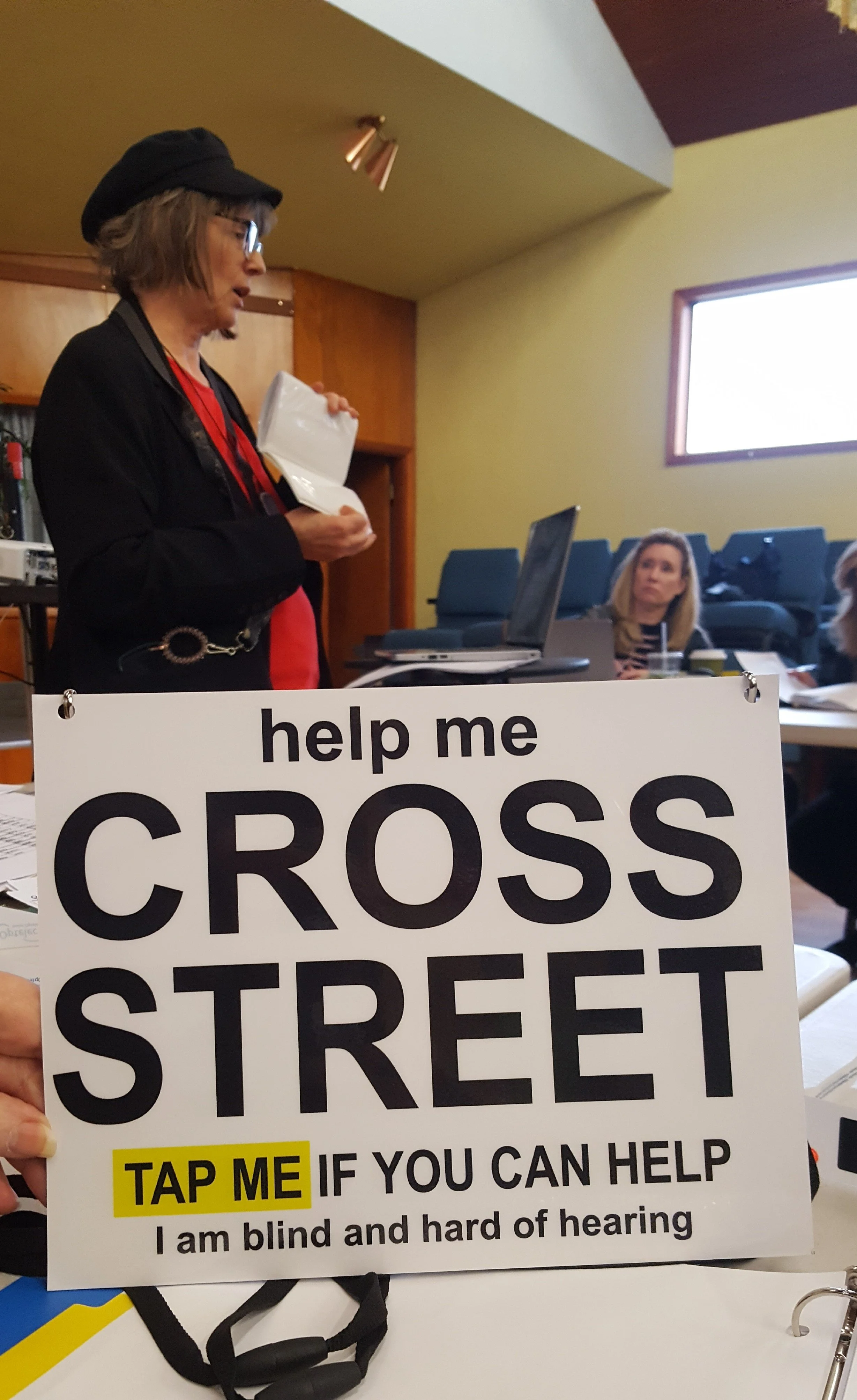
This summer, Portland State University and the Helen Keller National Center shared research on touch-based orientation and mobility (O&M) for travelers who are DeafBlind, as part of DeafBlind Awareness Week and its theme, Connected by Touch. I was honored to join the panel as a person who is deafblind: legally blind and hard of hearing to connect the findings to everyday life.
The research is framed around teaching strategies that provide cues other than speech, issues with technology and bluetooth use, and provided proof that deafblindness need not prevent independent safe travel. But underneath it is a lesson that reaches well past the crosswalk: how to communicate in noisy environments quickly and safely. Regardless of the level of hearing or blindness. Yet, it doesn’t mean that every deafblind person can travel anywhere, without careful attention to skills, and each environment.
When psychologists, counselors, and physical therapists interact with patients/clients who have some usable hearing and vision, need to understand that hearing and vision not always reliable hearing and vision. They may also be able to help process fears around being touched, or not being safe. Or perhaps use the information to empower clients if a system is saying that safe, independent travel is not possible. For it certaintly is, as long as the mobility specilist is aware of using touch, smell, temperature and many other cues, besides just hearing. In addition, several strategies using technology to communiate with the hearing/ sighted public are possible. Such as receiving texts, and reading it with a braille display. The world is much much accessible these days. But often times, the teachers or other professionals may not be up to date on the possibilities or techniques.
Why It Matters
Noise doesn't just make speech quieter; it makes it ambiguous. "No" and "go" can sound identical. "First Street" and "Fir Street" can send a traveler down the wrong route. In a clinic or gym, a misheard instruction during a transfer or a balance exercise isn't a small thing.
For a person with combined vision and hearing loss, how well they hear can change dramatically from one moment to the next, depending on background noise, fatigue, and how their hearing aids are set. A client who followed you easily last week may struggle today. That isn't inattention—it's the condition.
And there's a cost most instruments never measure: mental energy. When a person is worried they might miss something important, they brace, they slow down, and they lose focus. Reliable access to information does the opposite. When I know information will reach me in a form I can actually use, I stop spending energy straining not to miss it—and have more left for the decision, the exercise, or the conversation in front of me.
One principle sits above every strategy below: touch is only helpful when it's expected and welcome.
Always ask before you touch, and never make contact—or approach from behind—without warning. Announce yourself, say what you're about to do, and let the person tell you where and how firmly they prefer to be touched. Preferences vary from person to person and even day to day. A startle in a clinic, a gym, or at a curb isn't just uncomfortable—it can be unsafe. Consent here isn't a formality; it's the foundation everything else rests on.
Practical Strategies You Can Use Right Away
Get closer, not louder. Moving nearer and lowering your pitch does more than raising your volume—it preserves the soft consonants (s, t, p, c) that carry meaning and cuts through background noise.
Agree on a few touch signals, and keep them consistent. For example: two slow taps = ready / go; a firm squeeze or several quick taps = stop / wait; a touch to the right shoulder = move or turn right. The exact signal matters far less than both of you understanding it the same way, every time.
Confirm the words that matter. For anything safety-critical, have the person repeat it back, spell it into their hand (if you both know the manual alphabet), or write it on their palm. Sound-alike words are where quiet errors hide.
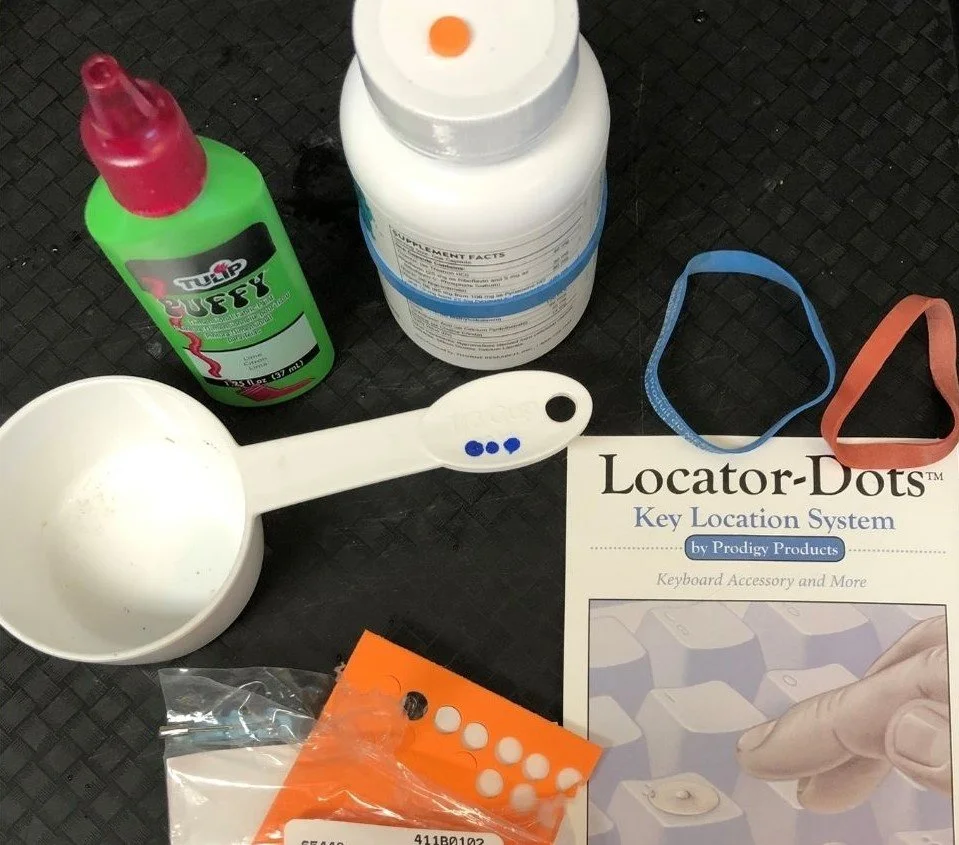
Build the picture by touch. A tactile map, a route traced on someone's back or arm, or a layout drawn on the palm can convey spatial information that spoken words in noise simply can't.
Treat fluctuating hearing as expected, not as effort. If a client seems to "tune out," check the environment and their fatigue before you read it as disengagement.
Be cautious with streaming tech in the community. Remote microphones and direct-to-hearing-aid streaming can sharpen a voice beautifully, but they often reduce the environmental sound—traffic, footsteps, room cues—a person relies on for safety and orientation. Great for a quiet conversation; risky at a busy intersection.
The Takeaway
For many travelers who are blind and hard of hearing, independence comes from combining touch, residual hearing, residual vision, environmental awareness, and good judgment. Touch is often the tool that organizes the information, reduces the ambiguity, and supports a confident decision. The same is true in your office or gym—so long as it always begins with permission and never a surprise.
Continuing the Mission of Access and Understanding
Adaptability for Life’s cultural competence - ethics continuing education courses provide engaging and practical skills in supporting their clients with vision/hearing loss.
Approvals - Accreditations:
OHA - Oregon Health Authority - Cultural Competence CE
CEP #18180 CA Board of Registered Nursing, Continuing Education Provider
NASW-OR Nat. Assoc. of Social Workers - Oregon Cultural Competence CE
CRCC - Commission on Rehabilitation Counselors Certification - Ethics CE
Who these courses are helpful for:
Nurses, Psychologist, LCSW, LFMT, PT, OT, SLP, ND, NP, PA, MD, DDS, LPC, Chiropractor, License Professional Counselor, Marriage and Family Therapist, Dentist, Dental Technologist, Dietitian, Emergency Medical Service Provider, Home Care Worker, Lactation Consultant, Long Term Care Administrator, Massage Therapist, Medical Imager, Midwife, Naturopathic Doctor, Occupational Therapist, Optometrist, Pharmacist, Polysomnographic Technologist/Respiratory Therapist, Social Workers, Caregivers and Families.
For those seeking to enhance their skills in communicating with those who have vision or hearing loss, consider enrolling.
2-Hour Cultural Competence CE: Effective Communication with Clients Who Are Hard of Hearing
4-Hour Cultural Competence and Ethics CE: Understanding the Diversity of Legal Blindness, Impacts & Solutions
6-Hour Cultural Competence and Ethics CE: Providing Culturally Competent Healthcare for Those Aging with Dual Sensory Impairments
Each course blends over 25 years of experience in rehabilitation counseling and disability services with lived insight and real-world examples. You’ll walk away with tools that help prevent social isolation, improve connection and communication, and foster hope—even in the face of progressive sensory loss.
What You’ll Gain
Strategies to prevent social isolation and despair
Tools to support clients experiencing progressive loss
Skills to improve communication and connection
Easy, low- or no-cost accessibility techniques
Real-world examples you can apply immediately
About the Instructor
Deb Marinos, MS, CRC, LPC, is a Certified Rehabilitation Counselor, Oregon Licensed Professional Counselor, and CMBM Mind-Body Skills Group Facilitator. She brings decades of teaching experience with health care professionals and other working with individuals navigating sensory loss and disability. Her courses are designed to be interactive, helpful, and will give you more comfort in your work.
Take the Next Step
If you’re ready to strengthen your skills, deepen your empathy, and make your practice more inclusive—join Deb and Olaf on this journey.
👉 Explore the Cultural Competence & Ethics accredited continuing education courses and sign up today at Adaptability for Life
Adaptability for Life LLC
21887 SW Sherwood Blvd. STE C
Sherwood, OR 97140
deb@adaptabilityforlife.com